Hemorrhoids
Sunday, September 6, 2009 by: sawan ModiBackground
Hemorrhoids are one of the most common causes of anal pathology. Subsequently, hemorrhoids are blamed for virtually any anorectal complaint by patients and medical professionals alike. Confusion often arises because the term "hemorrhoid" has been used to refer to both normal anatomical structures and pathological structures. In the context of this article, "hemorrhoids" refers to the pathological presentation of hemorrhoidal venous cushions.
Hemorrhoidal venous cushions are normal structures of the anorectum and are universally present unless a prior intervention has taken place. Because of their rich vascular supply, highly sensitive location, and tendency to engorge and prolapse, they are common causes of anal pathology.1 Symptoms can range from mildly bothersome, such as pruritus, to quite concerning, such as rectal bleeding, and while it is a common condition diagnosed in clinical practice, many patients are too embarrassed to ever seek treatment. Consequently, the true prevalence of pathologic hemorrhoids is not known.2
Even though hemorrhoids are responsible for a large portion of anorectal complaints, it is important to rule out more serious conditions, such as other causes of GI bleeding, before reflexively attributing symptoms to hemorrhoids.3
Pathophysiology
Hemorrhoidal venous cushions are a normal part of the human anorectum and arise from subepithelial connective tissue within the anal canal.
Present in utero, these cushions surround and support distal anastomoses between the superior rectal arteries and the superior, middle, and inferior rectal veins. They also contain a subepithelial smooth muscle layer, contributing to the bulk of the cushions. Normal hemorrhoidal tissue accounts for approximately 15-20% of resting anal pressure and provides important sensory information, enabling the differentiation between solid, liquid, and gas.
Most people contain 3 of these cushions. Although classically described as lying in the right posterior (most common), right anterior, and left lateral positions, this combination is found in only 19% of patients. Hemorrhoids can be found at any position within the rectum.
Hemorrhoids are classified by their anatomic origin within the anal canal and by their position relative to the dentate line.
- Internal hemorrhoids develop above the dentate line from embryonic endoderm. They are covered by the simple columnar epithelium of anal mucosa and lack somatic sensory innervation and are therefore painless.
- External hemorrhoids develop from ectoderm and arise distal to the dentate line. They are covered by stratified squamous epithelium and receive somatic sensory innervation from the inferior rectal nerve rendering them painful when irritated.
Anatomy of external hemorrhoid. Image courtesy of MedicineNet, Inc.
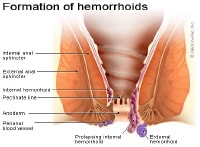
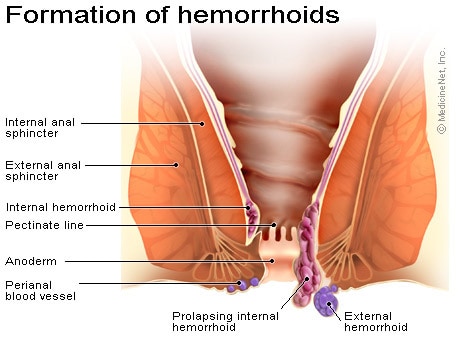
- Mixed hemorrhoids are confluent internal and external hemorrhoids.
Venous drainage of hemorrhoidal tissue mirrors embryologic origin:
- Internal hemorrhoids drain through the superior rectal vein into the portal system.
- External hemorrhoids drain through the inferior rectal vein into the inferior vena cava.
- Rich anastomoses exist between these 2 and the middle rectal vein, connecting the portal and systemic circulations.
Most symptoms arise from enlarged internal hemorrhoids. Abnormal swelling of the anal cushions causes dilatation and engorgement of the arteriovenous plexuses. This leads to stretching of the suspensory muscles and eventual prolapse of rectal tissue through the anal canal. The engorged anal mucosa is easily traumatized, leading to rectal bleeding that is typically bright red due to high blood oxygen content within the arteriovenous anastomoses. Prolapse leads to soiling and mucus discharge (triggering pruritus) and predisposes to incarceration and strangulation.
Most clinicians use the grading system proposed by Banov et al in 1985, which classifies internal hemorrhoids by their degree of prolapse into the anal canal. This system both correlates with symptoms and guides therapeutic approaches.
- Grade I hemorrhoids project into the anal canal and often bleed but do not prolapse.
- Grade II hemorrhoids may protrude beyond the anal verge with straining or defecating but reduce spontaneously when straining ceases.
- Grade III hemorrhoids protrude spontaneously or with straining and require manual reduction.
- Grade IV hemorrhoids chronically prolapse and cannot be reduced. They usually contain both internal and external components and may present with acute thrombosis or strangulation.
Frequency
United States
Prevalence of symptomatic hemorrhoids is estimated at 4.4% in the general population.
Race
Patients presenting with hemorrhoidal disease are more frequently Caucasian, from higher socioeconomic status, and from rural areas.
Sex
No predilection is known, although men are more likely to seek treatment. However, pregnancy causes physiologic changes that predispose women to developing symptomatic hemorrhoids. As the gravid uterus expands, it compresses the inferior vena cava, causing decreased venous return and distal engorgement.
Age
External hemorrhoids occur more commonly in young and middle-aged adults than in older adults. The prevalence of hemorrhoids increases with age, with a peak in persons aged 45-65 years.

